
Identify: Find At-Risk Youth
Screening is an essential aspect of suicide prevention. Universal screening identifies risk in a broader population that may not have clear risk within a general population of youth. This can be done within certain parameters such as age or setting, but is often broader and not focused on screening individuals with certain risk factors. Targeted screening, however, focuses on youth with some level of risk - such as a presenting behavioral health concern - risk screening occurs within a group that already has an elevated risk due to the nature of their presentation.
Depending on your setting and capacity, you may consider starting with one approach for screening and expanding your screening as feasible and as needs dictate, knowing that many youth who experience suicidal ideation may not present with a behavioral health concern or see a behavioral health provider. Universal screening in primary care offices, mental health practices, and emergency departments can ensure youth with elevated risk are identified and receive mental health support. Furthermore, it provides an opportunity for education and awareness for youth and families even when screening does not identify risk
A Comprehensive Approach
Additionally, there are regulatory requirements that may dictate screening practices in your setting. The American Academy of Pediatrics (AAP) recommends universal screening for youth ages 12+. For youth ages 8-11, screening is recommended when clinically indicated such as presenting for behavioral problems. AAP does not recommend screening youth under age 8 if warning signs are present. These are also Joint Commission guidelines that require screening over age 12 in emergency and hospital settings.
There are many evidence based screening tools that can assist in implementing a screening protocol. In most settings this is the CSSR, or ASQ. These screening tools are embedded in many electronic health records as well to ease and streamline suicide screening. At times, the PHQ-9, item-9, may be used as a screen for suicide risk. Although the PHQ-9 is a well validated and easy-to-use depression screen, it serves as a poor screener of suicide risk and should be supplemented by the ASQ or CSSRS to provide more high fidelity suicide risk screening in youth.
Once a screening plan has been developed, it is essential to think about Suicide Assessment. The focus of screening is to identify those at risk. The purpose of assessment is to determine the level of risk and clarify the nature of the risk. There are several evidence-based tools to support risk formulation and clinical assessment to support clinical decision making and connecting youth and families to the appropriate level of care. Two commonly used assessment tools include:
- Brief Suicide Safety Assessment (BSSA) (Conducting a Brief Suicide Safety Assessment)
- Suicide Assessment Five Step Evaluation and Triage (SAFE-T) (SAFE-T (Suicide Assessment Five-Step Evaluation and Triage) Flier)
The electronic medical record provides many opportunities to integrate risk screening and assessment as well as creating care pathways to track risk and promote communication. Engage also explores the evidence-informed practices that can be implemented to support youth and families during crisis including lethal means safety and collaborative safety planning.
Evidence-based Assessment
Utilizing a standardized suicide risk assessment is essential for informed clinical decision-making and determining the appropriate level of care. A comprehensive assessment goes beyond screening to confirm the presence and severity of suicide risk, identify imminent danger, and evaluate both risk and protective factors. This process helps clinicians understand the context of suicidal thoughts or behaviors, guide individualized treatment planning, and ensure timely interventions that align with the patient’s level of need. Standardized tools, such as the Columbia Suicide Severity Rating Scale (C-SSRS) or SAFE-T, promote consistency across providers, reduce bias, and support documentation that enhances continuity and quality of care.
Risk factors
Risk factors are static and dynamic characteristics or experiences that research has shown to impact suicide risk. Risk factors can support clinical decision making to understand what acute behavior changes or stressors may be present The following tool provides a mnemonic to recall common risk factors and support during a clinical assessment.
IS PATH WARM:
Ideation - threatened or communicated
Substance abuse - excessive or increased
Purposelessness - No reasons for living
Anxiety - Agitation/Insomnia
Trapped - Feeling there is no way out
Hopelessness
Withdrawing - From friends, school, society
Anger (uncontrolled) - Rage, seeking revenge
Recklessness - Risky acts, unthinking
Mood changes - dramatic, sudden change
Jacobs, D. G., & Klein-Benheim, M. (2021)
Risk Formulation
Risk formulation provides an opportunity to integrate information from the assessment to conceptualize risk level and again inform treatment planning. A risk formulation explores static and dynamic risk factors as well as protective factors. A risk assessment explores factors that can be modified in an individual’s environment and supports that can be activated to reduce risk. Oftentimes, risk is conceptualized as low, medium, and high with relevant interventions at each risk level to mitigate risk and promote safety. When reflecting on risk, the goal is to ensure safety in the least restrictive environment.
The model of risk formulation shared here was developed to reflect on the patient’s past, present, and future. The model assists in creating a narrative that includes the patient's current circumstances, how certain behaviors, beliefs, thoughts, actions, have come to be, how they have impacts on the patient’s life. It also explores available resources that can support in maintaining safety as well as acute changes in the future that may impact risk. The model focuses on identifying interventions that can modify risk to support in developing the most appropriate plan for patients with suicidal thoughts. The inclusion of foreseeable changes reflects on what factors to monitor to continue assessing how risk may change in the future.
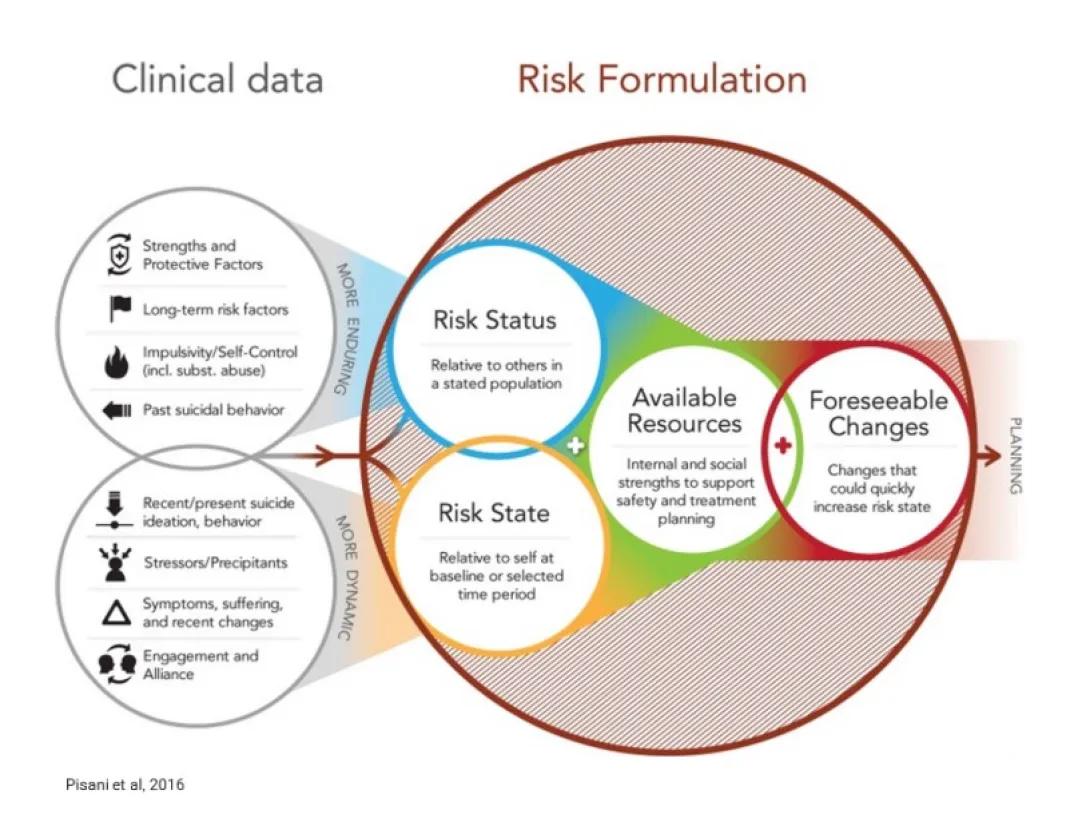
This image is a three-part overlapping circle diagram showing how clinical data and risk formulation combine to determine overall risk status. On the left, a gray circle labeled Clinical Data lists factors such as strengths and protective factors, acute stressors, psychiatric history, and recent behaviors. In the center, a large overlapping area labeled Risk Formulation combines information from the other sections to assess current and future risk. On the right, a white circle labeled Available Resources includes items such as coping skills, family support, and access to care. Where all areas overlap, a central section labeled Risk Status represents the clinical judgment of immediate and foreseeable risk, guiding care planning and safety decisions.
More Resources
FREE CSSRS Training for Individuals and Systems - The Columbia Lighthouse Project
Screening: Implementing a suicide prevention care pathway | PCMH Colorado
C-SSRS Screener Training - English (USA) | Columbia University Center for Suicide Risk Assessment
AMA Practical strategies for managing suicidal ideation and reducing risk
Preventing Suicide in Emergency Department Patients | Zero Suicide EDC
Suicide and Suicide Risk in Adolescents
Liwei HL, Lee J, Rahmandar MH, Sigel EJ. Pediatrics, 2024, 153(1).
DOI: 10.1542/peds.2023-064800.
Suicide prevention training: self-perceived competence among primary healthcare professionals
Solin P, Tamminen N, Partonen T. Scandinavian journal of primary health care, 2021, 39(3), 332-338.
doi: 10.1080/02813432.2021.1958462
Universal Suicide Screening Is Feasible and Necessary to Reduce Suicide
Goldstein GJ, Boudreaux, ED. Psychiatric Services, 2023, 74(1), 81-83.
DOI: 10.1176/appi.ps.202100625
Current Status of Suicide-Focused Assessment and Treatment: An Online Resource for Clinicians
Jacobs DG, Klein-Benheim M. Stop a Suicide, 2023.
Reformulating Suicide Risk Formulation: From Prediction to Prevention
Pisani AR, Murrie DC, Silverman MM. Academic Psychiatry, 2016, 40(4), 623–629.
doi: 10.1007/s40596-015-0434-6
Ask Suicide-Screening Questions (ASQ): A Brief Instrument for the Pediatric Emergency Department
Horowitz LM, Bridge JA, Teach SJ, Ballard E, Klima J, Rosenstein DL, Pao M. Archives of Pediatrics & Adolescent Medicine, 2012, 166(12), 1170-1176.
DOI: 10.1001/archpediatrics.2012.1276
Validation of the Ask Suicide-Screening Questions (ASQ) for adult medical inpatients: A brief tool for all ages
Horowitz LM, Snyder DJ., Boudreaux ED, He JP, Harrington CJ, Cai J, Claassen CA, Salhany JE, Dao T, Chaves JF, Jobes DA, Merikangas KR, Bridge JA, Pao M. Psychosomatics, 2020, 61(6), 713-722.
DOI: 10.1016/j.psym.2020.04.008
Validation and feasibility of the Ask Suicide-Screening Questions (ASQ) among pediatric medical/surgical inpatients
Horowitz, LM, Wharff EA, Mournet AM, Ross AM, McBee-Strayer S, He J, Lanzillo E, White E, Bergdoll E, Powell DS, Merikangas KR, Pao M, Bridge JA. Hospital Pediatrics, 2020, 10(9), 750-757.
Validation of the Ask Suicide-Screening Questions (ASQ) with youth in outpatient specialty and primary care clinics
Aguinaldo LD, Sullivant S, Lanzillo EC, Ross A, He JP, Bradley-Ewing A, Bridge JA, Horowitz LM, Wharff EA. General Hospital Psychiatry, 2021, 68, 52–58.
DOI: 10.1016/j.genhosppsych.2020.11.006
Universal pediatric suicide risk screening in a health care system: 90,000 patient encounters
Roaten K, Horowitz LM, Bridge JA, Goans CR, McKintosh C, Genzel R, Johnson C, & North CS. Journal of the Academy of Consultation-Liaison Psychiatry, (2021), Jul-Aug;62(4), 421-429.
DOI: 10.1016/j.jaclp.2020.12.002
The importance of screening preteens for suicide risk in the emergency department
Lanzillo EC, Horowitz LM, Wharff EA, Sheftall AH, Pao M, Bridge JA. Hospital Pediatrics, 2019, 9(4), 305–307.
Assessment of selective and universal screening for suicide risk in a pediatric emergency department
DeVylder JE, Ryan TC, Cwik M, Wilson ME, Jay S, Nestadt PS, Goldstein M, Wilcox HC. JAMA Network Open, 2019, 2(10).
DOI: 10.1001/jamanetworkopen.2019.14070
Identification of at-risk youth by suicide screening in a pediatric emergency department
Ballard ED, Cwik M, Van Eck K, Goldstein M, Alfes C, Wilson ME, Wilcox HC. Prevention Science, 2017, 18(2), 174-182.
SAFE-T Suicide Assessment Five Step Evaluation and Triage | SAMHSA Library
Screening for Suicide Risk in Clinical Practice | American Academy of Pediatrics
Identify & Address Suicide Risk Using Epic Tools | Zero Suicide EDC
Ask Suicide-Screening Questions (ASQ) Toolkit - National Institute of Mental Health (NIMH)
Current Status of Suicide-Focused Assessment and Treatment 2022 at McLean Hospital
Understanding and Preventing Youth Suicide | Duke Psychiatry