Aortic Stenosis (Pediatric)
Aortic Stenosis (Pediatric)
What is aortic valve stenosis?
Aortic valve stenosis is a narrowing of the aortic valve. This forces the heart to work harder to pump blood through the valve opening into the aorta and to the rest of the body. Stenosis can weaken the heart and cause other problems.
Aortic Valve with Stenosis
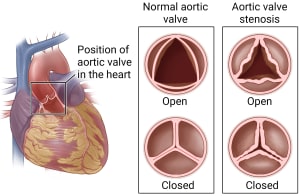
Normal aortic valve. A normal aortic valve opens fully to let blood flow into the aorta. The aortic valve has three flaps that work like a one-way gate. When the heart pumps, the aortic valve opens to allow oxygen-rich blood to flow from the left ventricle into the aorta. When the heart rests between beats, the aortic valve closes to keep blood from flowing backward into the heart.
Aortic valve stenosis. With aortic valve stenosis, the valve cannot open as wide as normal. Because the valve does not open as wide, the heart must work harder to pump blood through the valve.
Our Approach
Significant aortic stenosis is relatively uncommon, affecting about 6 of every 1,000 babies born, occurring more often in boys. It can occur alone (without other heart problems) or in association with bicuspid aortic valve, coarctation of the aorta, ventricular septal defect, mitral valve abnormality, and less commonly with atrial septal defect or complete atrioventricular septal defect. C.S. Mott Children’s Hospital is an international referral center for children with complex congenital heart disease. Our expertise in diagnosing and treating aortic stenosis includes specialization in fetal diagnosis and intervention as well as treatment and long term care for children diagnosed as infants.
Appointment Information
Our expertise in diagnosing and treating aortic stenosis includes specialization in fetal diagnosis and intervention as well as treatment and long term care for children diagnosed as infants. For more information on our programs and services, or to make an appointment, please call 1-877-475-6688.
Congenital Heart Center
An international referral center for children with complex congenital heart disease, our Congenital Heart Center is one of the largest and best pediatric heart programs in the U.S.
What are the symptoms of severe aortic valve stenosis in newborns?
Symptoms depend on how much narrowing there is in the valve. If there is only a little narrowing, there may be no symptoms.
When the narrowing is more serious, symptoms may include:
- A blue tint to the skin, lips, and fingernails.
- Fast breathing.
- Sweating while feeding.
- Not eating well.
- Being fussy a lot of the time.
How is mild aortic valve stenosis in newborns diagnosed?
Your doctor may hear abnormal heart sounds, such as a heart murmur, when examining your newborn.
Your doctor will order tests to find the cause of abnormal sounds or of symptoms. The most common test used to find this problem is called an echocardiogram, or "echo" for short. It uses sound waves to make an image of your baby's heart.
Your baby may have other tests, such as an EKG (electrocardiogram) or a chest X-ray. Another test may look at the amount of oxygen in the blood.
Prenatal Diagnosis: Fetal diagnosis of aortic stenosis is made by an echocardiogram of the baby's heart and can be made as early as 16 weeks into the pregnancy. An echocardiogram of the heart is done when a possible problem is identified during a routine prenatal ultrasound or because of a family history of congenital heart disease. The Fetal Diagnosis and Treatment Center offers comprehensive fetal diagnosis and treatment alternatives for unborn babies with aortic stenosis.
Symptoms: Symptoms of aortic stenosis are related to the degree of narrowing, leakage, and the presence of other heart problems. Mild aortic stenosis usually does not cause heart-related symptoms. More severe aortic stenosis may cause chest pain that is related to exercise, decreased stamina, palpitations or "skipping beats", and/or fainting. Undetected aortic stenosis can cause sudden death during vigorous physical exertion. Critical aortic stenosis in an infant can cause congestive heart failure with symptoms of poor feeding, rapid breathing, clammy sweating, lethargy, and/or irritability.
Physical findings: Aortic stenosis is often diagnosed due to the presence of a heart murmur. Infants may have symptoms of congestive heart failure as described above as well as weak pulses.
Medical tests: The gold standard for diagnosis is an echocardiogram. Cardiac catheterization is done if there are any questions not clearly answered by the echocardiogram and may also be done for therapeutic purposes, that is, to perform a balloon dilatation or angioplasty.
How is aortic stenosis treated?
For select patients diagnosed with aortic stenosis prenatally, fetal intervention can be an option. For children diagnosed after birth, or for babies for whom fetal intervention was not an option, treatment is determined by many factors including the location of the narrowing, severity of narrowing, associated cardiac problems, symptoms, age, and size. Valvar aortic stenosis can be treated surgically or by balloon dilation, a procedure done in the cardiac catheterization lab. For the most part, other types of aortic stenosis are treated surgically. These procedures are done to open up the area of obstruction to decrease the amount of work the left ventricle has to do to get blood out to the body. This helps to protect the heart muscle from overwork and development of heart failure and/or abnormal heart rhythms.
Aortic stenosis often progresses over time. Balloon angioplasty may be the only intervention required but is often used as a temporary means to delay open-heart surgery. This procedure is done in the heart catheterization laboratory. During the procedure, catheters (thin plastic tubes) are placed into the large blood vessels in the legs and gently guided to the heart. The catheter tip is placed across the aortic valve and the balloon tip is inflated. The balloon gently dilates the narrowed area. The incidence of complications is low and includes damage to the femoral artery, bleeding, perforation, and aortic valve leakage.
This procedure is a type of repair to the aortic valve in which the valve itself is stretched to allow better blood flow. During surgical valvotomy, an incision is made down the center of the breastbone. The heart is stopped for a brief period of time while the body is supported with a heart lung bypass machine (ECMO). The defect is then fixed by making an incision into the ascending aorta where it exits the left ventricle. An instrument called a dilator is then placed through the aorta and through the opening of the aortic valve stretching it. Progressively larger dilators are used until the valve is opened as much as possible without overstretching the valve which would allow it to leak blood backwards into the ventricle.
Sometimes the aortic valve is too narrow or too leaky to repair. When this happens the aortic valve will eventually need to be replaced. The goal is to identify when the valve function is poor enough to cause overwork for the heart, but before there is permanent damage. This is done through the history and physical examination as well as heart tests done during routine clinic visits. There are several types of valve replacement procedures and the choice of which operation is best for a child is decided through discussions with the parents, the pediatric cardiologist, and the pediatric cardiac surgeon. Valve replacements alone are not always enough to relieve the narrowing out the ventricle.
Sometimes the whole area leading out of the ventricle to the aorta is too small. The supporting structure of the valve, called the valve annulus, may be too narrow even if the leaflets are opened up as far as possible. In these cases the valve replacement is performed with a procedure called a Konno procedure. This involves enlarging the left ventricular outflow tract and the valve ring. It is done through an incision into the outflow tract of the right ventricle and the septum or wall between the right and left ventricles. A patch is placed in this area that enlarges it. The Konno procedure can be done with any type of aortic valve replacement.
Subvalvar stenosis can be caused by a discrete membrane or by thickened muscle. Repair for discrete membranous stenosis is done to prevent damage to the aortic valve and to preserve left ventricular function. An incision is made down the center of the breastbone and the heart is stopped for a brief period of time while a heart-lung bypass machine supports the body. An incision is made in the aorta and the surgeon looks through the valve to visualize the membrane. The membrane is cut away along with a tiny pie shaped wedge of muscle. This is called membrane resection with myectomy and decreases the chances that the membrane will grow back. Muscular subaortic stenosis is a more diffuse narrowing that sometimes involves the mitral valve.
The operation is performed in the same manner as discrete subaortic stenosis using the heart lung bypass machine. The surgeon incises the aorta and looks through the aortic valve to cut away the thickened muscle tissue. Care is taken to avoid the mitral valve structures. This type of narrowing is more difficult to treat and another operation to enlarge the entire left outflow tract may be required at a later time.
An incision is made down the center of the breastbone and the heart is stopped for a brief period of time while a heart lung bypass machine supports the body. The surgeon makes an incision along the length of the narrowing in the aortic wall. A patch is then placed into the area where the incision was made to open the area and relieve the narrowing. The size and length of the patch is determined by the degree of narrowing of the aorta.
Frequently Asked Questions
Like most heart defects, aortic stenosis does not have an adverse effect until after a baby is born. The health effects of aortic stenosis are related to the degree of the narrowing, valve leaks, and if there are other heart defects. The degree of narrowing is measured as the pressure difference across the aortic valve, which is referred to as the gradient. The higher the gradient, the greater the problem, since the left heart has to work much harder to pump blood to the body. Based on the gradient, aortic stenosis is diagnosed as either trivial, mild, moderate or severe. Critical aortic stenosis is a term used in newborns with very severe narrowing , requiring treatment soon after birth. Over time, if the problem is not treated, this overwork causes a thickening of the heart muscle called ventricular hypertrophy. Eventually, the muscle becomes damaged resulting in left-sided heart failure and abnormal heart rhythms.
When the aortic valve is affected, there may be leaking of the valve in addition to the narrowing. Terms used to describe the severity of valve leakage include trivial, mild, moderate, and severe. The more the valve leaks, the harder the heart and the left ventricle have to work to pump blood out to the body. The combination of significant leakage and narrowing can cause a great deal of stress on the heart. The natural history of aortic stenosis is that it tends to become more severe over time. For this reason, periodic visits to a pediatric cardiologist are important. If the narrowing is trivial and caused by a bicuspid aortic valve it may not progress. In a baby born with critical aortic stenosis, the opening is so small that the heart cannot pump enough blood to meet the baby's needs.
Unless the problem is treated early, the baby will develop problems with shock and congestive heart failure. A medication called prostaglandin may be used to keep the ductus arteriosus patent or open. The ductus arteriosus is a small blood vessel that connects the pulmonary artery with the aorta and provides a way for blood to get out to the body. The blood that exits the heart by the ductus arteriosus bypasses the lungs so the baby may look a little blue. Children with aortic stenosis are at increased risk for subacute bacterial endocarditis (SBE). This is an infection of the heart caused by bacteria in the blood stream. It can occur after a dental or other medical procedure and can largely be prevented by a dose of antibiotic prior to the procedure.
Exercise recommendations are best made by a patient's doctor so that all factors can be included in the decision. Children with aortic stenosis can participate in recreational physical activities but are usually restricted from competitive and vigorous athletic activities. If the aortic stenosis is trivial, they may be permitted to participate in competitive athletics but will need to see their cardiologist regularly to make sure that the narrowing has not progressed.
Overall, the outlook for people with aortic stenosis is very good. Since it is a lifelong problem that tends to progress over time, people with aortic stenosis need to see a cardiologist on a regular basis.
Locations
-
Congenital Heart Center | Brighton Center for Specialty Care 7500 Challis Rd
Entrance 1, Level 2
Brighton, MI 48116-9416Get Directions -
Congenital Heart Center | C. S. Mott Children's Hospital 1540 E Hospital Dr
Floor 11 Reception C
Ann Arbor, MI 48109-4284Get Directions -
Michigan Heart and Vascular Specialists | Burns Professional Building 560 W Mitchell St Ste 400
Petoskey, MI 49770-8895Get Directions -
Pediatric Cardiology Clinic | Munson Healthcare Pediatric Specialty Clinics 106 S Madison St
Traverse City, MI 49684-2320Get Directions -
Pediatric Cardiology Clinic | Trinity Health Michigan Heart 5325 Elliott Dr Ste 201
Ypsilanti, MI 48197-8633Get Directions -
Pediatric Cardiology Clinic | Trinity Health Oakland Hospital Medical Office Building
44555 Woodward Avenue, Suite 105
Pontiac, MI 48341Get Directions -
Pediatric Cardiology Clinic | U-M Health Sparrow Professional Building 1200 E Michigan Ave Ste 715
Ste 715
Lansing, MI 48912-1832Get Directions -
Pediatric Cardiology | Beltline Health Center - U-M Health West 1310 East Beltline Ave SE
Grand Rapids, MI 49506Get Directions -
Pediatric Cardiology | MyMichigan Medical Center Alpena 1501 W Chisholm
Alpena, MI 49707Get Directions -
Pediatric Congenital Heart Clinic | Northville Health Center 39901 Traditions Dr
Floor 2
Northville, MI 48168-9493Get Directions -
UP Health System - Marquette 850 West Baraga Ave.
Marquette, MI 49855Get Directions
News & Stories

Expert complex heart surgery team saves baby with rare genetic heart condition
Specialized local care gives baby with severe heart condition a stronger start before surgery
How to use an AED in a cardiac emergency

Fontan patient inspires as pediatric cardiology fellow
How lifesaving care after teen’s sudden cardiac arrest made motherhood possible years later