Thyroid Cancer
Thyroid Cancer
What is thyroid cancer?
Thyroid cancer is the growth of abnormal cells in your thyroid gland. These cells often form small tumors called nodules. But most thyroid nodules aren't cancer and don't cause harm.
There are several different types of thyroid cancer. The treatment for thyroid cancer is often successful with the right treatment plan.
Thyroid and parathyroid glands
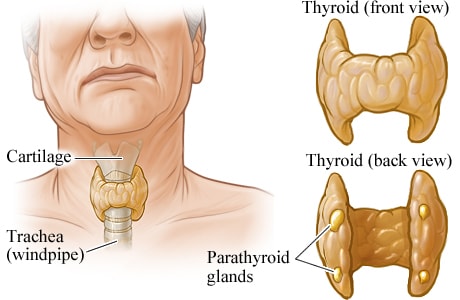
The thyroid is a butterfly-shaped gland that lies in front of the windpipe (trachea), just below the voice box (larynx). The thyroid gland uses iodine from food to make two thyroid hormones that regulate the way the body uses energy.
The parathyroid glands are four tiny glands located behind the thyroid gland. The parathyroid glands produce a substance (parathyroid hormone) that helps control the amount of calcium in the blood.
What are the types of thyroid cancer?
There are different types of thyroid cancer. They are based on what the cells look like under a microscope. Your treatment will depend on which type of thyroid cancer you have.
These include:
- Papillary thyroid cancer. This is the most common type of thyroid cancer. It's often only found in one lobe of the thyroid.
- Follicular thyroid cancer. It's found more often in countries where people don't get enough iodine from food.
- Hürthle cell cancer. This is a much less common type. It tends to spread to the lymph nodes in the neck.
- Medullary thyroid cancer. This isn't very common. One type occurs mostly in adults. The other type is inherited and often develops during early childhood.
- Anaplastic thyroid cancer. This is very rare. It's a very aggressive cancer that grows rapidly and is almost always fatal.
Other cancers that can start in the thyroid include lymphoma and sarcoma.
Appointment Information
The Endocrine Oncology Program offers diagnosis and treatment for those with thyroid cancer. If you have been diagnosed, or suspect you have thyroid cancer, patients, please call 734-647-8902.
Healthcare professionals, please contact our M-LINE service: 800-962-3555.
What are the symptoms of thyroid cancer?
Many people don't have any symptoms when they are diagnosed with thyroid cancer. This cancer is often found when an imaging test, like a CT scan, is done for another reason.
When thyroid cancer grows, it may cause these symptoms:
- You may get a lump or swelling in your neck. This is the most common symptom.
- You may have pain in your neck and sometimes in your ears.
- You may have trouble swallowing.
- You may have trouble breathing or have constant wheezing.
- Your voice may be hoarse.
- You may have a frequent cough that is not related to a cold.
It's important to note that nearly all thyroid cancers have little to no symptoms; and lab tests for thyroid cancer often come back negative (even when there is cancer). The best screening method -- and the best course of action should you display any of the above symptoms -- is to have your doctor check your neck on a regular basis.
What are the risk factors for thyroid cancer?
A risk factor is anything that affects a person’s chance of getting a disease such as cancer. Different cancers have different risk factors.
But risk factors don’t tell us everything. Having a risk factor, or even several risk factors, does not mean that you will get the disease. And many people who get the disease may have few or no known risk factors. Even if a person with thyroid cancer has a risk factor, it is very hard to know how much that risk factor may have contributed to the cancer. There is no known prevention. Awareness of risk (such as previous radiation therapy to the neck) can allow earlier diagnosis and treatment.
- Gender and age
It's unclear why, but thyroid cancers (like almost all diseases of the thyroid) occur about 3 times more often in women than in men.
Thyroid cancer can occur at any age, but the risk peaks earlier for women (who are most often in their 40s or 50s when diagnosed) than for men (who are usually in their 60s or 70s). - A diet low in iodine
Follicular thyroid cancers are more common in areas of the world where people’s diets are low in iodine. In the United States, most people get enough iodine in their diet because it is added to table salt and other foods. A diet low in iodine may also increase the risk of papillary cancer if the person also is exposed to radioactivity. - Radiation
Exposure to radiation is a proven risk factor for thyroid cancer. Sources of such radiation include certain medical treatments and radiation fallout from power plant accidents or nuclear weapons. Having had head or neck radiation treatments in childhood is a risk factor for thyroid cancer. Risk depends on how much radiation is given and the age of the child. In general, the risk increases with larger doses and with younger age at treatment.
Can thyroid cancer be inherited?
An abnormal gene has been found in patients with some forms of thyroid cancer, such as medullary thyroid cancer. If this cancer is diagnosed, the patient may have been born with a certain abnormal gene which may have led to the cancer. Family members may have also inherited this abnormal gene. Tests have been developed to determine who has the genetic defect long before any cancer appears. It is standard in the Multidisciplinary Endocrine Oncology Program to offer genetic counseling and a complete genetic evaluation to some of our thyroid cancer patients. For this reason, we work closely with the Cancer Genetics Clinic and include these clinicians on our tumor board.
Being diagnosed with a condition that causes cancer in the patient or in the patient’s family can influence how doctors treat patients. More importantly, genetic evaluation can identify other types of cancer the patient is at risk for, and physicians will be able to recommend other screening methods for early detection of these cancers. The diagnosis of a familial cancer syndrome also allows for the identification of other family members who might be at risk for developing the same types of cancer. Family members at risk then have the chance to discuss preventive measurements and screening protocols which are geared towards finding tumors at an early stage where they can be treated with greater success.
- Hereditary conditions and family history
Several inherited conditions have been linked to different types of thyroid cancer, as has family history. Still, most people who develop thyroid cancer do not have an inherited condition or a family history of the disease:- Medullary thyroid cancer:
About 1 out of 3 medullary thyroid carcinomas (MTCs) result from inheriting an abnormal gene. These cases are known as familial medullary thyroid carcinoma (FMTC). - Other thyroid cancers
People with certain inherited medical conditions have a higher risk of more common forms of thyroid cancer. Higher rates of thyroid cancer occur among people with uncommon genetic conditions such as:- Familial adenomatous polyposis (FAP):
People with this syndrome develop many colon polyps and have a very high risk of colon cancer. They also have an increased risk of some other cancers, including papillary thyroid cancer. - Cowden disease:
People with this syndrome have an increased risk of thyroid, endometrial (uterine), and breast cancers. The thyroid cancers tend to be either the papillary or follicular type. - Carney complex, type I:
People with this syndrome may develop a number of benign tumors and hormone problems. They also have an increased risk of papillary and follicular thyroid cancers.
- Familial adenomatous polyposis (FAP):
- Medullary thyroid cancer:
How is thyroid cancer diagnosed?
Some patients find that they have a thyroid lump (nodule) when a family member or healthcare provider notices a lump on their neck. In other cases, thyroid lumps are found when getting tested for some other health problem.
How will they decide if my lump is cancerous?
To start, your doctor (endocrinologist) will take your medical history. Then you’ll have a physical exam. Your doctor will look at the size and firmness of your thyroid and for any enlarged lymph nodes in your neck. Next, you will have a thyroid ultrasound. At UM we use the latest techniques in ultrasound so that our doctors can gather the most information to find out if your lump is cancerous. You may have other tests such as lab work and a biopsy. For a biopsy, a sample of cells from the area of concern is removed and looked at under a microscope. The most common type of biopsy to look for thyroid cancer is called fine needle aspiration. To make your visit more convenient, your doctor may do the ultrasound and biopsy at your first visit.
How is thyroid cancer treated?
At the Rogel Cancer Center, we use a team approach (called multidisciplinary care). This means that we have members from many healthcare professions reviewing and talking about your medical condition and treatment choices.
After going through the diagnosis process, if we are worried your lump is cancerous, surgery is often recommended. Some lumps stay in the unknown (indeterminate) grouping after testing. Your doctor will discuss choices with you about this grouping of lumps. Thyroid hormone therapy may also be used to stop cancer cells from growing. If thyroid cancer is advanced when diagnosed, treatment may also include chemotherapy or radiation therapy. It is very rare to need chemotherapy. Radioactive iodine is the most common form of radiation therapy used to treat thyroid cancer after surgery and is very well tolerated.
What are my choices for surgery?
Surgery for thyroid cancer usually involves removing the whole thyroid gland (total thyroidectomy), but other options may be appropriate for some patients. The University of Michigan is one of only a few health systems in the U.S. that offers video-assisted surgery for the treatment of thyroid disease. This may be a choice in certain cases, including patients with unknown lumps that need to be removed.
Your surgeon will talk with you about the right choice for you. We use the most advanced surgical techniques along with intraoperative nerve monitoring. This technique helps to maintain the quality of your voice.
What is radioactive iodine therapy and how is it given?
After surgery, some patients get radioactive iodine treatment (also known as radioiodine, I-131 or RAI). This treatment is used to get rid of any very small (microscopic) amounts of left over thyroid cancer. If your doctor orders radioactive iodine for your cancer, you will take the medication by mouth (pill or liquid).
What is thyroid hormone replacement therapy?
After you have ended your radioactive iodine treatment, you will take daily thyroid hormone replacement therapy. The dose will be carefully monitored and adjusted by the team taking care of your thyroid cancer.
What is the treatment for advanced thyroid cancer?
At times thyroid cancer in the neck cannot be treated by surgery and radioactive iodine therapy. Sometimes thyroid cancer spreads (metastasizes) beyond the neck to other organs. If this happens, these metastases may not be treatable by surgery and radioactive iodine therapy. Some patients with these advanced forms of thyroid cancer can be treated with external beam radiotherapy. External beam radiation uses high doses of radiation to destroy cancer cells and shrink tumors.
In addition, new forms of oral (taken by mouth) chemotherapy have been shown to be effective in advanced cases of thyroid cancer, though chemotherapy is rarely curative. If your cancer cannot be treated by external beam radiation or chemotherapy, we offer clinical trials. The care of patients with advanced thyroid cancer is discussed at our weekly Tumor Board meetings.
What about long term follow-up care?
Your doctor will want to see you on a regular basis to make sure your cancer has not come back (recurrence). At these visits your medical history will be reviewed and you will have a physical exam, paying close attention to the neck area. An ultrasound of the neck is sometimes done to check for lumps or cancerous lymph nodes.
If needed, other imaging tests will be done. Blood tests also are important to help determine if thyroid cancer has recurred and to see if the thyroid hormone therapy is working. Administration of a drug called Thyrogen is sometimes used to help evaluate for recurrences. All patients who have had their thyroid removed need thyroid hormone replacement with levothyroxine.
Locations
-
Endocrine Oncology Clinic | Rogel Cancer Center 1500 E Medical Center Dr
Floor B1 Reception A
Ann Arbor, MI 48109-5911Get Directions -
Otolaryngology Clinic | Taubman Center 1500 E Medical Center Dr
Floor 1 Reception A
Ann Arbor, MI 48109-5312Get Directions
Doctors

Keith Andrew Casper, MD
Clinical Associate Professor
Otolaryngology

Debbie Wan Hua Chen, MD
Clinical Assistant Professor
Endocrinology, Internal Medicine

Nazanene Helen Esfandiari, MD
Clinical Professor
Endocrinology, Internal Medicine

David WA Forner, MD, MSc, FRCSC
Clinical Assistant Professor
Otolaryngology

Paul Glenn Gauger, MD
Professor
Surgery, Surgical Critical Care
Thomas James Giordano, MD, PhD
Professor
Anatomic Pathology

Megan Rist Haymart, MD
Professor
Endocrinology, Internal Medicine

Molly Elaine Heft Neal, MD
Clinical Assistant Professor
Otolaryngology

David Thomas Hughes, MD
Clinical Associate Professor
Surgery

Shruti Jolly, MD, MBA
Clinical Professor
Radiation Oncology







Providers

Elizabeth A Hesseltine, NP
Advanced Practice Nurse
Nurse Practitioner
News & Stories

What should you know before starting a GLP-1?

Long friendship inspires urology resident fund
Researchers create new path to target hard-to-drug prostate cancer protein
Study explains how colorectal cancer cells maintain high iron levels
2 Rogel members recognized by American Thyroid Association
