Primary Hyperparathyroidism
Primary Hyperparathyroidism
What is primary hyperparathyroidism?
Primary hyperparathyroidism is a condition that causes elevated calcium levels (hypercalcemia) in the bloodstream, due to the parathyroid glands secreting too much parathyroid hormone (PTH). In a healthy body, when the calcium level is high, the PTH level should be very low or undetectable. The body doesn't need the parathyroid glands to produce any PTH when the calcium levels are high in the blood stream. It is by far the most common type of hyperparathyroidism, and in 85% of patients the disorder is caused by a single abnormal gland.
What are the causes of primary hyperparathyroidism?
Primary hyperparathyroidism is caused by abnormal growth of cells within the parathyroid gland. In most cases a single gland is involved, but 15-20% of the time multiple glands are abnormal. In 99% of cases, these are non-cancerous growths. Parathyroid cancers often present with very high calcium levels (often >13mg/dL) and have slightly different appearances on imaging studies. Parathyroid disease can be due to genetic abnormalities, passed from one family member to another. Genetic syndromes affecting the parathyroid glands include multiple endocrine neoplasia syndromes (MEN) I and IIA.
Appointment Information
To make an appointment with one of our physicians, please see our locations section and choose the facility that's most convenient for you or your loved one.
What are the symptoms of primary hyperparathyroidism?
Signs and symptoms of primary hyperparathyroidism can range from none or very mild to extremely serious. Measurable signs of abnormally functioning parathyroid glands may include:
- Brittle bones (osteopenia and osteoporosis) which can lead to fractures
- Kidney stones and decreased kidney function
- Increased acid secretion in the stomach with may lead to gastritis or ulcers
- Pancreatitis
- Heart disease
How is primary hyperparathyroidism diagnosed?
Since the symptoms of primary hyperparathyroidism can be non-existent or very mild for a long time, the condition is often discovered as part of routine blood testing done at the time of a yearly routine physical examination or at the time of evaluation for another unrelated medical condition. If a patient goes to a physician already experiencing some of the above signs or symptoms, blood tests can be ordered to check for primary hyperparathyroidism. Common tests ordered to check for primary hyperparathyroidism include serum and/or ionized calcium, parathyroid hormone, basic metabolic panel, phosphorous, 25 hydroxy vitamin D, and 24-hour urine for calcium and creatinine.
How are abnormal parathyroid glands located?
A number of different types of imaging studies may be used to locate abnormal parathyroid glands, but even if someone has the disease, an abnormal gland or multiple abnormal glands may not show up on the imaging study. Primary hyperparathyroidism is a biochemical (lab) diagnosis, so parathyroid surgery should not be dismissed if an abnormal gland is not identified by imaging. Often, the glands hide behind other structures and can’t be seen until structures can be moved out of the way during surgery. The most common imaging studies obtained are ultrasound and sestamibi scans, but CT, MRI, and other types of imaging studies may also be ordered.
Doctors

Nevin Nuray Ajluni, MD
Clinical Assistant Professor
Endocrinology, Internal Medicine
Cristina Alvarado Nieves, MD
Clinical Assistant Professor
Endocrinology, Internal Medicine

David Tyler Broome, MD
Clinical Assistant Professor
Endocrinology, Internal Medicine

Debbie Wan Hua Chen, MD
Clinical Assistant Professor
Endocrinology, Internal Medicine
Tae-Hwa Chun, MD, PhD
Associate Professor
Endocrinology, Internal Medicine
Gregory Adam Clines, MD, PhD
Associate Professor
Endocrinology, Internal Medicine
Farah Daneshvar, DO
Clinical Assistant Professor
Endocrinology, Internal Medicine

Liselle Douyon, MD
Clinical Assistant Professor
Endocrinology, Internal Medicine

Nazanene Helen Esfandiari, MD
Clinical Professor
Endocrinology, Internal Medicine

Nada Fanous, MD
Clinical Assistant Professor
Endocrinology, Internal Medicine









News & Stories

Supplementing with peptides: Good for extra pep or a needless step?

Teenage patient receives treatment for papillary thyroid cancer

New study reveals a missing step in a weight control pathway that could be targeted for obesity treatment
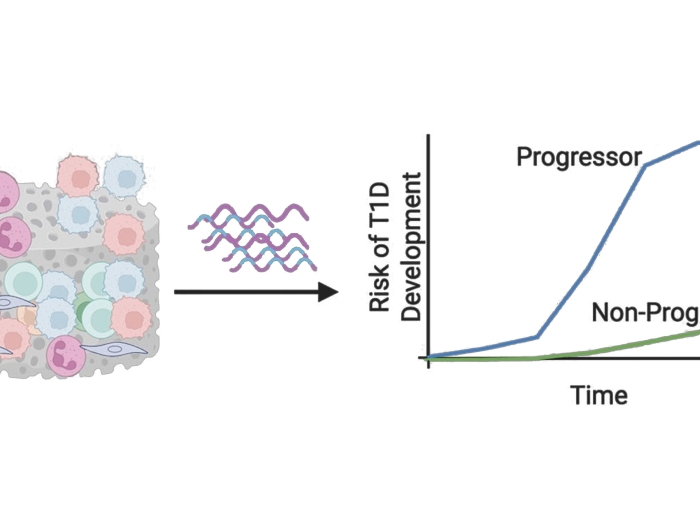
New hope for early diabetes detection

Podiatry clinic helps patient with recurring foot ulcer
