Achilles Tendon Problems
Condition Basics
What is the Achilles tendon?
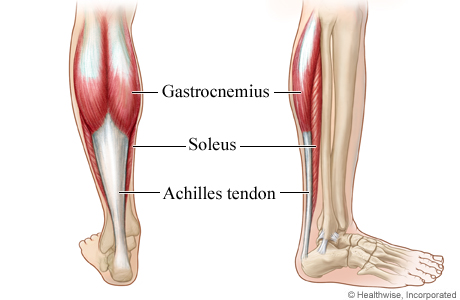
The Achilles tendon connects the calf muscle to the heel bone. The calf muscle is actually two muscles, the gastrocnemius muscle and the soleus muscle. The soleus lies underneath the gastrocnemius.
The Achilles tendon is the largest tendon in the body. It allows you to rise up on your toes and push off while walking or running.
What are some Achilles tendon problems?
The two main injuries are:
- Achilles tendinopathy.
This refers to tiny tears (microtears) in the tissue in and around the tendon. These tears are caused by overuse. This is often called Achilles tendinitis.
- Achilles tendon tear or rupture.
An Achilles tendon also can partly tear or completely tear (rupture). A partial tear may cause mild or no symptoms. But a complete rupture causes pain and sudden loss of strength and movement.
Problems with this tendon may seem to happen suddenly. But in most cases they are the result of many tiny tears in the tendon that have happened over time.
Other conditions can affect the Achilles tendon area. They include:
What are the symptoms?
Symptoms of Achilles tendinopathy may include:
- Pain in the back of the heel, in the Achilles tendon area. Pain may be mild or severe. It may come on slowly or may only occur when you walk or run. Swelling may occur.
- Tenderness in the Achilles tendon area. You may notice it more in the morning.
- Stiffness that goes away as the tendon warms up with use.
- Decreased strength and movement, or a feeling of sluggishness in the leg.
Symptoms of an Achilles tendon tear may include a sudden, sharp pain. Most people feel or hear a pop. You may have swelling and bruising. You may not be able to point your foot down or stand on your toes. Some people with partial tears may not have any symptoms.
How are these problems diagnosed?
To diagnose Achilles tendon problems, such as tendinopathy or a tear, most doctors ask questions about your past health and do a physical exam. The exam includes checking for tenderness, watching how you walk and stand, and comparing the range of motion of your two legs.
Other tests may be done to clarify a diagnosis or to prepare for surgery. These tests include:
- Ultrasound. It may be used to see if there is a tendon tear or signs of tendinopathy.
- X-rays. These are used to check the heel bone.
- MRI scan. It may be used to check the tendon for signs of tendinopathy or a tendon tear. An MRI is also used to evaluate the heel bone.
How are Achilles tendon problems treated?
Treatment for mild Achilles tendon problems like Achilles tendinopathy includes rest, over-the-counter pain medicine, and stretching exercises. You may need to wear well-cushioned shoes and change the way you play sports. Orthotic shoe devices can help reduce stress on the tendon. You may get physical therapy. In some cases, surgery may be needed.
Surgery may be used to treat a torn tendon. A cast, splint, brace, walking boot, or other device may also be used. These devices keep the lower leg and ankle from moving. Rehab follows both of these treatments. Exercise, in either physical therapy or a rehab program, can also be used.
How can you help prevent an Achilles tendon problem?
Most Achilles tendon injuries occur during sports. If you had an Achilles tendon problem in the past, it's even more important to try to prevent another injury. Make sure to:
- Warm up. Before any sport or intense activity, gradually warm up your body by doing 5 to 10 minutes of walking or biking.
- Cool down and stretch. After intense activity, gradually cool down with about 5 minutes of easy jogging, walking, or biking. Then do 5 minutes of stretches.
- Avoid any sport or intense activity that you aren't in condition to do.
- Wear shoes that cushion your heel during sports or any strenuous activity.
- Wear heel pads or other orthotics that are designed to reduce stress on the Achilles tendon.
Current as of: July 17, 2023
Author: Healthwise Staff
Clinical Review Board
All Healthwise education is reviewed by a team that includes physicians, nurses, advanced practitioners, registered dieticians, and other healthcare professionals.

